1. What Actually Happens During an Abortion?
Abortion is common, but it’s something we rarely talk about. So let’s clear up the biggest mystery first: what actually happens during an abortion? A provider guides us through, step by step.
Guest: Dr. Meera Shah, family medicine physician, Chief Medical Officer of Planned Parenthood Hudson Peconic, and author of You’re the Only One I’ve Told: The Stories Behind Abortion.
Music by Lily Sloane, logo by Kate Ryan.
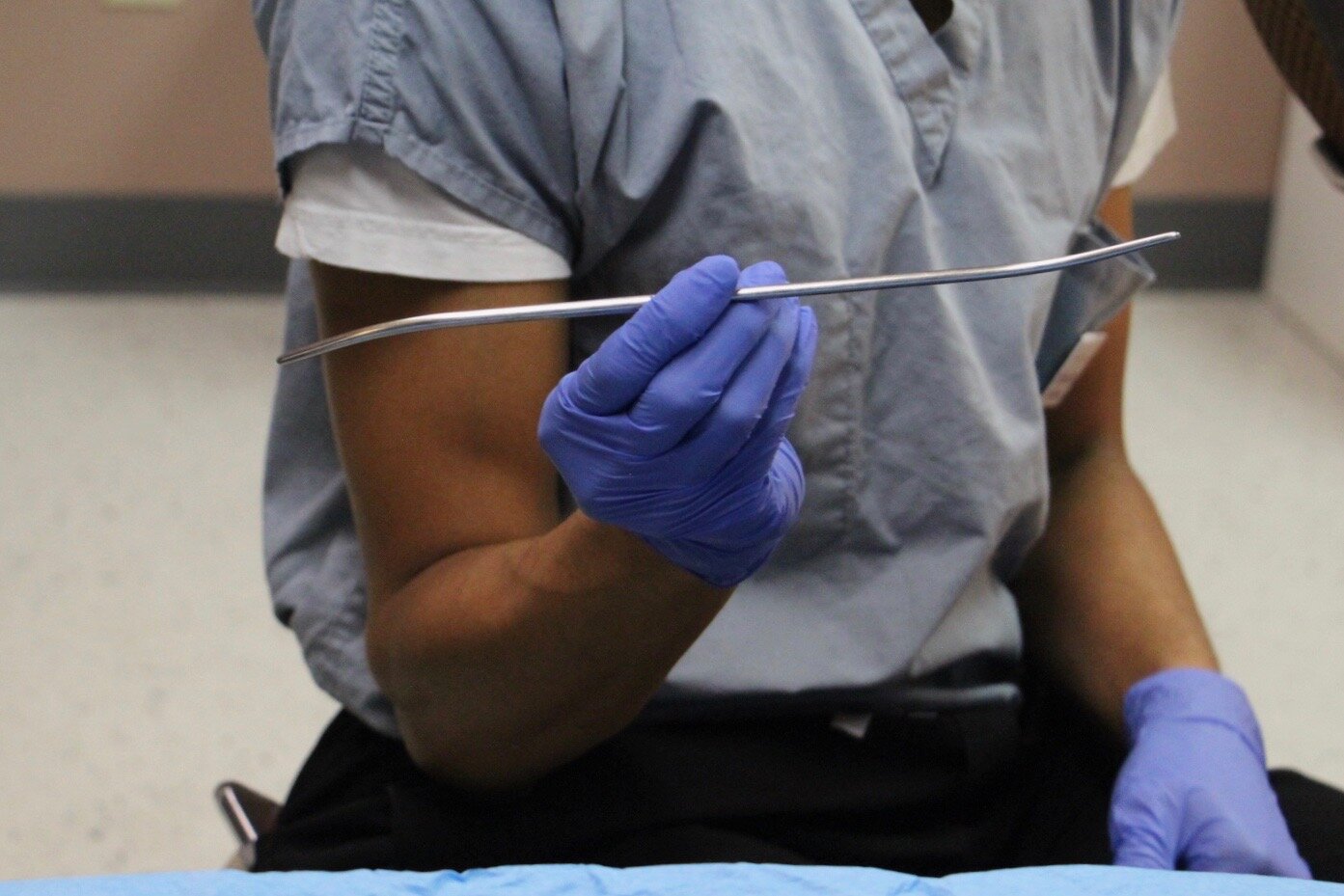
For an illustration of some of the medical instruments Dr. Shah mentions in this episode, see the photos below by Robin Marty, author of Handbook for a Post-Roe America. They’re part of her collection of abortion stock photos. Full episode transcript below photos.









Garnet Henderson [00:00:01] Welcome to ACCESS, a podcast about abortion. I'm your host, Garnet Henderson.
[intro music plays]
Garnet Henderson [00:00:39] Abortion is common. In the United States, one in four women will have an abortion during her lifetime, and many trans men and nonbinary people have abortions, too. That means that you almost certainly know someone, and probably more than one person, who's had an abortion—if you haven't had one yourself. But abortion is something that many people just don't talk about. At least, not outside the context of political debates. On this podcast, I want to demystify abortion, and give you the information you need to really understand the things you're hearing about in the news. So today, we're clearing up the biggest mystery first: What actually happens during an abortion? An abortion provider is going to guide us through, step by step.
Dr. Meera Shah [00:01:29] My name is Dr. Meera Shah. I'm a board-certified family medicine physician and I am the chief medical officer of Planned Parenthood, Hudson Peconic here in New York. I'm also a fellow with the Physicians for Reproductive Health.
Garnet Henderson [00:01:43] Dr. Shah is also the author of a new book, out this week, called You're the Only One I've Told: The Stories Behind Abortion. According to the Guttmacher Institute, which compiles the most comprehensive statistics on abortion in the United States, the vast majority of abortions in this country—over 88 percent—take place in the first trimester, or the first 12 weeks of pregnancy. Over 65 percent take place at or before eight weeks. So, during this time, there are two options for someone who wants an abortion: medication abortion, which can be done largely at home, or an in-clinic aspiration abortion. We'll talk about medication abortion first. Medication abortion, often referred to as the abortion pill, is FDA approved for use up to 10 weeks of pregnancy. After its initial approval in 2000, it was a little slow to take off, but now its popularity is growing rapidly. In 2017, for example, 39 percent of all abortions in the U.S. were done with medication. That's a 10 percent increase just from 2014. One misconception I hear a lot is that the abortion pill and the morning after pill are the same thing. But this isn't true. And here's the difference. There are two types of morning after, or emergency contraceptive pills. In the U.S., these are sold under the brand names Plan B and Ella. These pills prevent pregnancy, primarily by delaying or preventing ovulation. They do not work to terminate existing pregnancies. Medication abortion does terminate pregnancy, using different drugs. So here's how it works.
Dr. Meera Shah [00:03:29] Medication abortion is a really safe way to end a pregnancy. It has a very, very low complication rate, like less than point five percent. And it involves a series of pills. The first pill is called mifepristone, and what it does is it blocks a hormone called progesterone. So progesterone is needed for a pregnancy to grow and to continue. But what mife does is that it blocks this hormone, thus preventing the pregnancy from continuing. So mife will end the pregnancy. But then it's not until a patient takes misoprostol, four tablets of misoprostol, they can put them in the cheeks, so two in each side, let them dissolve for 30 minutes, swallow the rest, or they can insert the four tablets in the vagina. And what the miso does is it induces cramping and bleeding, which kind of organizes the expulsion of the pregnancy. So again, mife will end the pregnancy and miso will cause expulsion of the pregnancy. Miso alone will end a pregnancy. It's about 80 percent effective in ending a pregnancy up to 10 weeks on its own. But mife does improve that efficacy. Patients take the mife at the office and then they take the miso at home. Within an hour or two, they should expect to experience the cramping and the bleeding. And the worst of it is for the first few hours. And then it just sort of trickles down and then they can experience some some spotting, some, you know, some bleeding for a few weeks until their body starts to regulate the monthly bleeding again.
Garnet Henderson [00:05:17] Dr. Shah says that patients usually manage the discomfort from cramping with high-dose ibuprofen. That's Advil. A week or two later, there's a follow up, to ensure that the abortion is complete. This either involves an ultrasound or checking for pregnancy hormones with a blood test or a special type of low-sensitivity home pregnancy test. Lots of people choose medication abortion precisely because it's done at home, where they feel comfortable. And many abortion providers would like to offer medication abortion via telemedicine. But there's a whole patchwork of state and federal regulations that make this difficult. And our next episode is actually devoted to this subject, so I'm not going to get too deep into it right now. But I will mention that, mifepristone, the progesterone blocker, is regulated under an FDA program called REMS. That stands for Risk Evaluation and Mitigation Strategies. It means that providers who want to prescribe mifepristone have to be registered with the drug manufacturer, stock it in their office, and dispense it to patients directly, among other requirements. So, they can't just write you a prescription to fill at a pharmacy. This is despite a wealth of evidence that medication abortion is safe. In fact, even the former FDA commissioner, who was head of the agency when mifepristone was approved, has come out to say that these regulations need to be rolled back. In July, the ACLU did manage to win an injunction blocking that in-person REMS requirement due to the pandemic. So providers in some states have been able to start mailing the pills to their patients instead of dispensing them in person. But the Trump administration has asked the Supreme Court to reinstate that in-person rule, and state laws make things even more complicated. Like I said, our next episode is a deep dove into telemedicine abortion and the COVID-19 pandemic, so for now, we're going to move on to aspiration abortion. Dr. Shah is going to mention several medical instruments here. If you want to get a better idea of what they look like, we have a great collection of photos on our website by Robin Marty, who, among many other things, is the author of a book called Handbook for a Post-Roe America. So take a look at those photos at apodcastaboutabortion.com. OK, like medication abortion, aspiration abortion involves cramping. So patients have a few different options for pain relief. They can take NSAIDs, like Advil or Aleve, and some patients opt for moderate sedation, which involves a low dose of a benzodiazepine or narcotic. Some health centers do offer deep sedation using Propofol, which is the same sedative that would be used for a procedure like a colonoscopy. But for first trimester abortions, this is uncommon.
Dr. Meera Shah [00:08:12] If the option is there, people tend to take it. So I think patients tend to choose a moderate sedation. But I will say, it's interesting, a lot of patients are like, 'Oh, that was so quick and easy, I don't feel like I needed that.' That said, I never try to deter people away from getting sedation, because if they want their experience to involve sedation, then I'm gonna be totally supportive of that. Even with moderate sedation, patients, they're not out. It's not like general anesthesia. They're, they're sedated, we've taken the edge off, but they're still able to follow commands and hear what I'm saying. So I'm guiding them through the process, if that is what they want. If they don't want me to say anything to them, I will not say anything to them. But many patients, I find, do want me to guide them through step-by-step, what's happening.
Garnet Henderson [00:09:01] So now we'll get into the procedure itself.
Dr. Meera Shah [00:09:03] So an aspiration procedure is very safe. Very, very low complication rate. And what it involves is a patient having a speculum exam, just like getting a pap smear, or a pap test, locating the cervix. The cervix is the opening to the uterus where the pregnancy is. So the uterus has the pregnancy and the cervix is the entry point to the uterus. We use an instrument called a tenaculum to stabilize the cervix.
Garnet Henderson [00:09:34] I'm interrupting here just to say that if you have an IUD, like I do, this might sound familiar, because these are the same steps a provider takes when they're getting ready to place an IUD. And for anyone who doesn't know, IUD stands for intrauterine device. It's a contraceptive device that's placed inside the uterus, and in many cases, if a person wants an IUD, it can actually be inserted on the same day they have their abortion.
Dr. Meera Shah [00:09:59] Anytime we're inserting or removing something from the uterus, we stabilize the cervix with an instrument called a tenaculum. And then we will apply some lidocaine around the cervix to numb up that canal, because similar to labor, we actually stretch the cervix to open a little bit so that we can then remove the pregnancy. And just that act of stretching the cervix with dilators can induce cramping. So we different size dilators to stretch the cervix slightly open, based on the number of weeks pregnant that they are.
Garnet Henderson [00:10:36] Cervical dilators used for first trimester abortions are small, typically no larger than the size of a pencil, or maybe your pinky finger.
Dr. Meera Shah [00:10:44] And then you can use two different types of aspirators. One is a manual vacuum aspiration. So it's this plastic device that's actually used all over the world. It's cheap. It's easy to use. That creates a nice suction. They are great little device. We insert a cannula into the uterus that corresponds to the number of weeks pregnant that the patient is. It's almost like a straw. And you insert that into the cervix, and then one end is in the uterus, the other end is outside of the body. And we attach the MVA to the other end where we release the suction. And then we remove the pregnancy. For patients who are more pregnant, and this is also a style thing. This really depends on the physician you talk to, because some physicians will always use the electric aspirator. Some will use the manual aspirator more than others. It really depends. But typically, for people who are a little bit more pregnant, we will use an electric aspirator, so an EVA, where we put a cannula into the cervix. So one end is in the uterus, one end is outside of the body. And then we attach tubing, which is then attached to a machine that we turn on. And it creates more suction to remove the pregnancy. The whole process takes anywhere from two minutes to four minutes. That's really it. And then afterwards, we evaluate the tissue to make sure that we are confident that all parts of the pregnancy have been removed. Sometimes we'll have an ultrasound in the examination room so that we can get a picture of the uterus after it has been emptied. And then we monitor for bleeding. We always check to make sure that the patient isn't bleeding. Usually they're not. And then we take them to the post-procedure room and give them a snack and some ginger ale. If they just received local sedation, meaning lidocaine around the cervix, they are just monitored for like 15, 20 minutes. And then if they have received moderate sedation, then we watch them for 30 to 45 minutes and then their escort will pick them up.
Garnet Henderson [00:12:54] This type of procedure is very commonly referred to as a surgical abortion. But many abortion providers are trying to move away from that. And here's why.
Dr. Meera Shah [00:13:05] It's not a surgery. We're not cutting. We're actually using an opening in the body that already exists. I know when counseling patients, they are oftentimes scared to choose the procedure because they think it's a surgery, because that's what it's been called for so long.
Garnet Henderson [00:13:20] You'll also hear this procedure referred to as a D&C. Again, this is common, but it's outdated. Dr. Shah explains why.
Dr. Meera Shah [00:13:29] D&C stands for dilation and curettage. So dilation, as I described, and then curettage. Basically, they used to go in with like an instrument kind of scrape. We use the aspiration, the suction technique just because it's really effective in removing the pregnancy, just that pressure.
Garnet Henderson [00:13:49] So that's why I'm using the term aspiration abortion. You'll also hear this called a vacuum aspiration or a suction abortion. They mean the same thing. Aspiration abortions are usually performed up until about 16 weeks of pregnancy, though this can vary a bit depending on the provider. After that, the most common abortion procedure is called a D&E, which stands for dilation and evacuation. D&E follows a lot of the same general steps as an aspiration abortion. First, the person having the D&E chooses the sedation level they're most comfortable with. Then, their cervix needs to be dilated, and it needs to dilate more than an aspiration procedure, so the process can take a little longer. Sometimes providers use something called an osmotic dilator, also known as laminaria or lams for short. Lams work by slowly swelling as they absorb water to dilate the cervix gradually. Medications may be used as well.
Dr. Meera Shah [00:14:49] Sometimes we'll give them miso, which I described is used for the medication abortion because miso what it does, it softens and opens the cervix. So we'll give miso, we'll insert lams to prep it and to minimize the amount of instrumentation we have to do of the cervix. And patients will sit with those inserted for some time to allow the cervix to open up. And then the procedure continues. And sometimes, and again, this is a style thing. Some patients will have that done the day before and then they'll come in the next day. It really just depends on how far along they are.
Garnet Henderson [00:15:24] So once the cervix is dilated, the pregnancy is removed. And this happens a little differently than in an aspiration procedure as well.
Dr. Meera Shah [00:15:32] So typically, after 16 weeks, there is no aspiration of the pregnancy. It's about removal with instruments of the pregnancy.
Garnet Henderson [00:15:43] The instruments used also vary depending on the provider, but generally, we're talking about a small forceps, which is a grasping tool, and/or a curette, which is like a very tiny spoon. Suction is often used as a final step. Once the provider is sure the uterus is clear, the patient spends some time in a recovery room and then heads home. Many states have attempted to limit access to abortion after the first trimester, some by banning D&E specifically. Only a handful of these bans have gone into effect, but more and more of these laws are being introduced across the country. This is one of the many abortion access battles that's making its way through our legal system. Now, sometimes later abortions are done using drugs that induce labor. This is called induction abortion, but it's far less common than D&E and it's even more variable, depending on the provider and the precise circumstances of the person who's having the abortion. So that's why you're not hearing about it in detail in this episode. But we are going to talk more about later abortion in future episodes. While later abortions are less common, there are lots of reasons why people need them, and they tend to be the most difficult—and costly—to access.
[music plays]
Garnet Henderson [00:17:00] So now you know what actually happens during an abortion. And remember, if you're still wondering what the heck a tenaculum, or a cervical dilator, or a vacuum aspirator is, you can see Robin Marty's photos of some of those things on our website. That, again, is apodcastaboutabortion.com. There's just one more thing I want to mention here. You heard Dr. Shah say several times that abortion is very safe. And I want to give you a better idea of what she means when she says that. One of the most comprehensive studies we have found that the overall complication rate from abortion was about 2.1 percent. But most of those complications were very minor and easily resolved. Serious complications, the kind that require treatment in an emergency room, happened less than one quarter of one percent of the time. That makes abortion safer than colonoscopy, wisdom tooth extraction, and tonsillectomy. It's also about 14 times safer than childbirth. I want to thank Dr. Shah for being my guest on this episode. We recorded this interview long before the COVID-19 pandemic began when everything, including my plan for this show, was very different. So I spoke with her more recently about what it's been like to continue providing abortion care during a pandemic. You're going to hear some of that conversation in our next episode, when we dive into telemedicine abortion, the COVID-19 pandemic, and what happened when some states used a public health emergency to temporarily ban abortion. So I hope you'll join us then.
[outro music begins]
Garnet Henderson [00:20:19] ACCESS is produced by me, Garnet Henderson. Our music is by Lily Sloane and our logo is by Kate Ryan. Special thanks this episode to Addie Henderson, Claire Tighe, and Alison Turkos. You can subscribe to ACCESS wherever you get your podcasts, and follow us on Instagram and Twitter at @accesspod. More information and a full transcript of this episode are available on our website, apodcastaboutabortion.com. This is a fully independent production, and if you're able to support the show, I would really appreciate it. You can contribute by visiting glow.fm/apodcastaboutabortion. That's also linked in the show notes. You can also really, really help out by leaving a rating or review, or better yet, sharing the show with your friends. Thank you, and see you next time.
[outro music ends]